Data analysis to find a simple investing strategy for decent returns by testing how well the stock market follows the Pareto principle.
Data source - (Dec - 30 - 2021) 5-year return on equity (ROE) data exported from the paid version of tickertape.in for the companies listed in Nifty 500.
Histogram for visualization showing number of companies vs percentage return.
Pareto Principle can be followed. 20% losers, and 80% winners in the portfolio can give an average 15% annual return in long term investing.
Optimization can be done based on various factors but that may not be necessarily useful.
For a hypothetical case of having the highest return possible on a portfolio of 15 stocks containing only top performers is 53% but surely finding such multi-baggers may be very difficult and even on making a dedicated effort on analysis only 1-2 such may be found for a portfolio of 15 stocks.
Note - Nifty 50 ETF gave 16% ROE (5 Y Avg)
PS - when insurance companies or big pharma may be working on insurance premium or drug pricing etc, data for normal distribution in a similar way on a representative population may become highly useful. Use and harm because of data depends on the purpose it's used for i.e. to maximize profit or to maximize access or somewhere in the middle.
While current efforts are towards adoption and interoperability to enable patient data access 24*7 globally as longitudinal record for their life journey, there isn't any technologically feasible and safe way but only debates and tiny projects around open access de-identified data which someday may get utilized at the global scale (even useful if scale is not so huge). The low hanging fruit may be firstly enabling the access to all research papers globally, or all data of clinical trials for better critical appraisal or atleast reporting of outcomes of all trials including those with negative outcomes. The most urgent goal is surely global equitable access of covid vaccines. The paragraph below is taken from project working on a real world scenario to alleviate human suffering with help of open access de-identified data, not in healthcare directly neither global scale but still surely useful.
"In almost every state, courts can jail people who fail to pay fines, fees, and other court debts—even those resulting from traffic or other non-criminal violations. While imprisoning someone for failing to pay a debt remains illegal on paper, these aggressive debt-enforcement tactics have led to the de facto reemergence of debtors’ prisons. Many believe that thousands of people across the country are jailed each year for unpaid fines and fees, but a dearth of data has made it difficult to rigorously assess and curb modern-day debt imprisonment practices. To address this data gap, we’re compiling an extensive database documenting debt imprisonment. Ultimately, we will anonymize the data and publish them for researchers, civil rights advocates, law enforcement officers, and other criminal justice stakeholders."
The NNT data available on thennt.com for cardiology speciality, visualized on logarithmic scale to give insight about various interventions. No bar drawn in case of none helped by the drug in given scenario based on available evidence. Purpose for drawing the visualizations was to understand the realistic range/expectation of effects from drugs.
Insights:
- 18 out of 48 have no effect.
- 3 have NNT 5 of less
- 6 have NNT 6 to 10
- 12 have NNT 11 to 50
- 6 have NNT 51-100
- 4 have NNT above 101
- 1 have NNT above 1500 i.e. Aspirin to prevent first heart attack or stroke.
FHIR - Fast Healthcare Interoperability Resources is getting adoption at tremendous speed and hence enabling scope for successful nationwide interoperability while also being easy to get started and implement. OpenEHR also solves the interoperability challenge as one of its features. While FHIR adoption and ecosystem is maturing in India, interoperability problem may be best tackled with it.
Combining OpenEHR with FHIR and clinical terminologies (eg. LOINC, SNOMED CT) is a possibility to build more powerful electronic medical records because of the Archetypes in OpenEHR.
"Archetypes define the possible clinical content, representing a model that originates from actual clinical practice. Archetypes have a governance boundary around them, essentially representing a clinical sign off that can be used to support the idea of a clinical data standard. One or more archetypes can then be used in a template that represents a specific clinical use case. A simple example could be the development of a Body Mass Index (BMI) app. In order to achieve this, we need three principle archetypes to capture height, weight and the BMI itself. The benefit of using these standard archetypes is that they can also be inserted into other templates that require the same clinical data. And when that data is stored in a common way, it can be queried and reused, reducing the burden of repeated data entry." 1
"Reuse of data - A key attribute of any clinical data repository is its ability to facilitate reuse for additional clinical requirements and for audit and reporting purposes. The Archetype Query Language exists to support this. AQL provides a means of performing queries on the CDR for individual or multiple records at either the patient or archetype level, maintaining data provenance and exporting for more advanced analysis where needed."1
While clinical terminologies help in analysing data, AQL provides another dimension of data analysis i.e. at patient/archetype level in much easier way.
fig 1 - example archetype
Conclusion -
Design choice of :
- using FHIR for Interoperability (across the globe).
- using OpenEHR Archetypes for data storage (writing to database and reusing in templates)
- AQL on CDR and clinical terminologies for more powerful analytics.
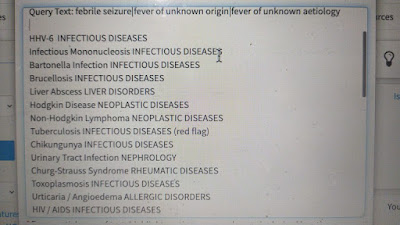
18 year old male, he had his first seizure at the age 5 when he was having High fever. By the age of 18 now he had 10 such episodes of seizure.
He gets this high fever every 3-6 months and temperature goes to 103-104 degree fahrenheit. He had adenoidectomy and Tonsillectomy 6 years back to prevent these recurring fever but it didn't help. Currently he is having similar fever again.
For his seizure he had - Valparin - 2008 - Tegrital-2012 - Levipil-2013 and currently he takes Levipil (levetiracetam) and since it started there were no more seizure episodes. He used to get hospitalized after seizure episodes and neck rigidity used to be there so csf analysis was done which had nothing significant, neither any pathology found in MRI and EEG. Severe Proteinuria happens during hospitalization phase which goes back to normal on recovery. Usually after 24 to 48 hrs of fever seizure happens. Sodium Valporate was taperd and stopped in 2010 ,but 2 months after that he again developed seizures without fever, Again in 2013 levipil was stopped but the following day he developed an episode of so the dosage was increased and we were advised to continue the medication further. These were the two instances when he got the episode without fever
During the same black Swan event, various decision makers (doctors) overused CT scans for screening covid and overused various drugs for prophylaxis and treatment while various guidelines and minimalist doctor's choose to go with symptomatology and conservative with home care unless needed otherwise.
All medical decisions are between a minimalist-maximalist range, like in quants case it's between nowcasting and forecasting. How to find the balance or at least mostly be on the winning side? (at least on winning side may not be acceptable in medical decision making, as having minimum losses “do no harm” is the first important rule not to be missed when caring for a patient.)
My understanding is, risk management is the key to finding the right balance which will help minimize losses, in quant field there are various objective tools for that, and same for the AI (and present day HI - human intelligence) is the way to go for medical decision making, so in medicine using techniques to find ADR, Anaphylaxis early and intervene early for them is important, evidence based rational use to prevent overtesting while also avoid undertesting and same way over treatment and under treatment. Also detecting suboptimal response of drugs in individual to find opportunity to replace with better alternatives if possible and even predicting what drugs may response better based on genotype/metabolomics/microbiome more easily and widely and other risk management strategies. These all are already known and application of these must increase towards finding the balance but still all these strategies together also may not guarantee a black swan / disaster in medicine but sometimes for the reward (clinical benefits) we have to take the remaining risk.
An example of black swans in medicine is PSA test misuse and many such examples exist there in medicine, which must be prevented by keeping strong focus on research (data generation , collection and analysis) for evidence and its appraisal.
The black swan / disaster in medicine may not be a sudden bad event, rather a bad practice not caught and corrected early.
IBS patient update - initially I was feeling bored and also wanted to change the topic rather than listen to tiny and probably useless points when she was speaking at very slow speed and I had to rush to read more for exam preparation but I tried keeping patience for sometime and what I got was something extremely amazing. She was slow as many stories she had lived like real life were going through her mind, where most if them were painful ones.. She was trying to evaluate them and make it in meaningful statement as how she is awake with eyes open but far far away from reality, feeling living in imagination which feels completely real and some moments are so slow as if time have stopped and this super slow scene stays there for long like many minutes or probably even an hour as she fails to keep track of real-time and these Stationary scenes gives her most amazing experience. Amazing in happy or sad way or what, can't explain clearly but may be can say the most powerful feelings. She detailed more about kind of stories she have lived but avoided giving much details, may be because fear of being judged, specially as I am a good friend now or also because risk of being Interfered as I needed to get back to study.. With details what beautiful thing I learnt was her "self hypnosis" Helping her to get big relief from chronic physical and emotional trauma and pain.
This show's a good opportunity for use of immersive tech like VR/AR/XR/MR against chronic pain (physical/emotional) management which has already started to become reality.
For a person practising self-hypnosis, it may be better to be guided by a professional who may help do better, safer and maybe less saddening ways. Interested to hear from trained clinical hypnosis practitioners or please share in comments if any relevant publications.
Self hypnosis = frugal, immersive (human tech).
Reply from RB sir - Amazing write up 👏 Reflective self hypnosis is a great idea toward a new tech supported therapeutic tool 👍
"It was recognized from the 1940s onwards that what was needed was a ‘health policy’ rather than a ‘disease policy’ as summed up by the director of the medical services Dr W. G. Wickremesinghe as early as 1945. Despite this ongoing acceptance of the benefits of preventive medicine the balance of government expenditure was overwhelmingly in favour of curative medicine as is the case in most other countries. One estimate of this balance in 1975 suggested that for every rupee spent on the curative sector only 12 cents was spent on prevention of disease and the promotion of health. This situation prompted the director of the Colombo Hospital to ask in 1970: “Was it more important to improve sanitation, nutrition, and health education and provide basic facilities for health and patient care for the masses of this country; or was it more important to go in for sophisticated and expensive programs like heart transplant units?” (Daily News, 3 Sept 1970). However, the hospitals were the visible symbol of Sri Lanka’s free health service and the symbol of modernity; switching resources to preventive public health was a highly politically contentious issue.
There were deep roots to the development of primary health care services in Sri Lanka and it represented at international level an example of what could be done without the levels of expenditure common in developed countries. Sri Lanka´s experience was an essential part of the debate on primary health care which took centre stage at international level in the 1970s. Furthermore, given the extent of its hospital based curative system it was also a perfect illustration of the limits of that model for low-income countries in the context of a burgeoning population and economic crisis. However, in the succeeding decades the challenge for Sri Lanka has remained that of finding the most effective route to reducing morbidity. This is now an ever more pressing priority with the demographic transition to an ageing population and the resulting double disease burden."
A learning portfolio which is much important aspect of medical education and currently improving in adoption across institutions in India. It is not something much different from journal's used by doctors in the last century and before. Analyzing the qualitative and quantitative data gives rise to insights and hypotheses and even helps to improve pattern recognition (both conscious and subconscious/intuition-based). Reflective learning is the most important aspect of creating a learning portfolio and I try to do the same using this blog as a learning portfolio.
Having a trading journal, analyzing why a trade is taken, what was the risk-reward and the outcome understanding it more by reflective learning and gaining insight is of similar high value in both domains. When this data is recorded and checked at the end of day/week/month along with P&L (preferably at month-end), it's auditing the trades and similarly in medicine also clinical audits are done which helps in improving the clinical outcomes.
Somewhat related to the risk-reward of a trade is the NNT and NNH data of an intervention. Based on the scenario we select risk and reward ratio while taking a trade, and similarly based on clinical scenario we select an intervention with an appropriate risk-reward ratio i.e. NNT , NNH and proceed with hope.
Sometimes the scenarios are unclear in trades and it's easy to not trade at that moment/time/day where there is an opportunity cost as a loss but may prevent a much bigger loss, but in medicine when the scenarios are unclear as in complex or rare undiagnosed cases, ignoring complexity is same as opportunity cost loss, but failing to find a diagnosis or suitable intervention is a helpless scenario. Hopefully, the more learning around patient-centred way and accessibility to those learning portfolios will help many more as have been already helping in a slower way by case reports published in journals.
To become a trader we need to learn fundamental and technical analysis and understand about market and economy, the more we know and practice, the better we may become. Along with the above knowledge we also need to develop skills in identifying opportunities (diagnosing), using the right strategy as position sizing, stop loss defence, monitoring, (intervention, dose, duration, monitoring, follow up, change in plan, ADR check, etc.)
And a few core principles like "never lose money" and it's equivalent in medicine as "do no harm" And all can be practised and visualized extremely fast in real-time with help of trades in the real market. This can be a great educational strategy to explain the decision science concepts in medicine.
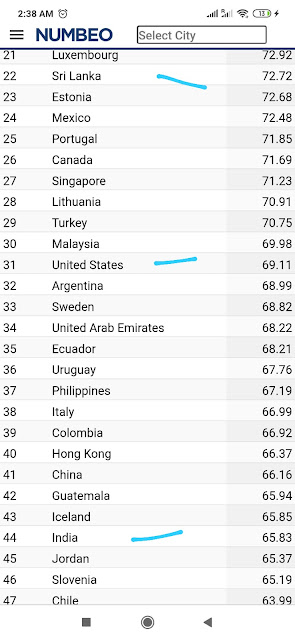
Iceland economy, and same globally, 2008 bubble, predicted by raghuram rajan in 2005 and similarly happened the dot-com bubble and many more.. One such bubble may be the hydroxychloroquine and similar eminence based, large scale and media promoted medications use for covid during the beginning which still being continued now to a great extent. The eminence based medicine even influenced official guidelines to a great extent and luckily the living guidelines /meta analysis got huge adoption to rule out the negative aspects.. The point to focus here is not the negatives of eminence medicine completely as when nothing was know about covid it was probably only way to go but as the world and research moved at super fast pace, it was more important to keep up with updates/data rather than keep playing blind and also to prevent misinformation based on updated information.
There are always some small/big bubbles, some eminence based guidance, biased eminence and evidence, and slow updates causing great damages. At an individual level overdiagnosis and overmedication is also one such problem to be managed actively by choosing wisely when to be a minimalist and when a maximalist, eg. In the recent flood of covid mild symptomatics, or hydroxychloroquine prophylaxis, etc. Where minimalist approach wouldn't have done any harm, specially when there was no data to support.
RB -
"One way to implement rational minimalism is to first identify the "parachute" intervention (the one that hasn't been tested in an RCT and yet every physician knows they can't do without, for covid recently, it was oxygen) and then decide about the other interventions keeping wishes of all the stakeholders around the patient in mind rather than aim at covering all therapeutic targets with rational but marginal efficacies, all the while remembering that it's the trillion cells in the body that would be responsible for 80% of it's healing with time rather than the chemicals or molecules we deliver.
In all this process the role of the doctor is very much like the man in this video
who strapped a 100 year old US citizen onto his shoulders and jumped out of the plane along with him till he landed safely.
Rational minimalism may drastically summarize the three goals of medical care into one, which is to "be with the patient" till he lands safely. It would rely on strong and well designed complex empathy straps to hold the patient, doctor (and the family) together all through the plunge in regular best case scenarios."
It's commonly said but now I also feel that the market is a war between bears and bulls and my (and every trader to be successful) target is to be with the stronger one at the moment to get some profit and exit. It's so best to follow the trend and avoid catching tops and bottoms.
I do mistakes frequently though, and one such mistake, when I tried catching the top, was when Delta variant started creating troubles in Europe recently as I was having the "intuition" based on medical knowledge as what it can do in the community at the national level and hence the economy. Sadly the trade was a failure initially and the market kept rising but after 2 days of big drawdown and losses in premium cost but finally, the market reversed and went down giving great profits. Similarly, when again I tried to catch the top but not with great logic, I failed badly.
Learning point I want to emphasize here is its good to follow the trend, as good to continue the treatment that is helping, but sometimes logic may suggest a different idea or what logical may not seem to be helping in short term (minutes/hours/days depending on timeframe) but great in long term, and balancing the care plan by good decision making there is an art. A good simple example is TB medication where in short term the ADRs create bigger troubles but in long term view, sticking to it while minimising ADR where possible may be the best thing, similarly weaning of a ventilated patient though uncomfortable in short term but great in long term, and in a complex scenario where lots of unknowns and huge uncertainty efforts on analysing the case data by taking more/better/detailed history, available knowledge base etc. May be better than focusing on batteries of tests. It doesn't mean tests are not important, but it means patient centred research, analysis and maybe also N of 1 trials are more important to be utilized.
👏you are opening a new way of looking at medicine and it is just at the right place at the right time.
Let's utilize this learning analogy to further the field of medicine 👏
RB - It's a breakthrough analogy 👏👏👏 Try reviewing the literature to see if anyone has had this analogy idea before.
Avi - Thanks a lot sir 🙏🙏 . I am having this thought since a few days that may be it becomes an educational strategy someday as checklists became from airline industry correlation.
no such literature sir. its commonly said that trading is like medical decision making as a wrong decision may destroy whole capital(like can kill a human)... but nothing more than that.. but here the discussion is from medical perspective, there is zero literature in pubmed and i didn't find also in gray literature.
After learning to play well with equity in various styles like scalping, intraday trading with and without heavy leverage. positional trading and swing trades, which range from low-risk low profit to high-risk high profit, i succeded managing some amount to cover my monthly expenses while also keeping my savings safe as it is. The market stabilized from the bull run and became sideways and in such case, good decisions become important as bad decisions can easily cause some money loss which is not during the case of a bull run where there is lots of freedom to make mistakes and still be in some profit (bull runs seems to be like self-healing / limiting diseases). Worst for these trading styles could be a bear (falling) market where there may be no profit and even the losses may break even with a long gap if they grow too much. There are derivatives which helps to make investments for trading in all kind of market scenarios, they are known as futures and options and they allow to make bets in both up down and range bound market to earn. Options are a very high risk money making instrument with great complexity but when utilizing its power, the real focus needs to be on a few key features like intrinsic value, delta and maybe just time decay also to some extent for practical purpose. Derivatives have more than 75% money of whole stock market of India and out of that 90% is just in the index options.
playing with derivatives, i lost 30% of capital while trying to learn, where major losses were on a single day when i made the intentional mistake of trading too aggressively with clear mind that either i will learn or leave this to may be neve do again (at least for a few years).. The day i lost 30% it was actually a 45% loss with 15% recovery, and being able to make recovery made me confident in trading with options. While option selling is the safest way and hedged option buying is some risk some profit, the option buying is the maximum and very fast profit making technique though it causes huge losses and at extreme speed.
within a week I recovered all losses and made my capital 1.5 times from what I had when started trading options.
Great success, and while options buying is said to be equivalent to gambling (can be better said as high risk high profit and uncertainty) I understood to utilize multiple factors to deal with uncertainty to some extent. What helps most in such high risk high uncertain scenarios was the real-time data, price action, and indicators. The Price action analysis is highly subjective while indicators are objective but all indicators are derived from price itself by applying some mathematical formula and all are lagging indicators compared to the price, and having this feeling and being able to profit better with price action, now my trading screen is much cleaner and not having multiple indicators anymore, just occasionally I add one or 2. This price action seems to be equivalent to the subjective and objective status of SOAP. Subjective as the overall price action now, an hour back, yesterday, this month etc.. and objective as the current real-time status, better if more complete and with more accuracy and in a form such that can be easily grasped by mind..
Another change is using different type of candles rather than the common heiken ashi candles, depending on the need of analysis. what i am using is heiken ashi sometimes and volume candle most of the time, it helps tract the real time movement with finer view of reality to understand what is happening in the market.
While trading options there are some index heavy weights too, i track them too and they are equivalent to the heavy weight objective markers that can make drastic impact on a patients health over time or suddenly eg. SpO2 in a case of covid pneumonia.
its the tape and tape reading is frequently used for trading, their won't be zeroes but real numbers of orders floating and hence the real game of supply and demand.
My trading terminal a while back with technical indicators overload and now simple but equally enjoyable ->
98% of retail investors make no profit over a duration of 1 year.
90% traders loose 90% money in 90 days.. (Trading and investing is a lil. Different but overall just a game to Make money).
2% who makes money, many times they are correct, evidence based, strategic, very good at managing risk, lucky, etc. (but that all are just 20% , a random)
And rest 80% game is played by time, helping them win sooner or later.. Simple best practices help them get time more strongly in their favour.
Good that we say EBM and whole science is 1% of knowledge, rest 99% yet to be discovered and that's where lots of good/bad (benefits and harms to patients) happen but it's mainly time game at play after applying all the little amount of deployable science we have (medical knowledge doubles every 72 days but deployable knowledge doesn't change so fast when we look both the best available evidence {1/2 goes wrong every 5 year} and available resources to help practice any among many of the best/better possible things.)
The technology software in world for data , evidence, and analytics (Bloomberg terminal) and the best (complexity ranging from zero to 100%) techniques as quant/algo or human mind (precision) have things that are futuristic in medicine like whole environment data , or whole past data (womb to tomb) etc. Are available but as human behavior/human psychology / mass psychology / mass psychology built in into the algorithms replacing humans, affect the stock prices alot, they are not exponentially efficient to be accurate at prediciting future price, nor exponentially efficient to generate higher returns..
And the catch is 1) into this image below
2) into inability of all these combined together and analysed with current analytics to capture the uncertainty of human mind/life & interactions in the biosphere.
- a screenshot of best software available
Do this very low level analytics help in making time in our favour?
- yes. Tremendously
Do simplicity win in long run
- yes. Without overcomplicating it can give decent returns and prevent big damages.
can time be an enemy too? (yes. especially when analytics is wrong. diagnosis or wrong harmful treatment may harm, and for diseases where prognosis is know to be bad as not much possible to do, then also time is enemy and in later case we may have no control)
not finding the triangle, it basically says, more advanced technique gives more reward but with more risk. so net gain is not exponentially high in general.
its very important skill to develop psychology to match with time game, else there will be again just losses/damages.
RB - 👍👏
data from the biosphere - climate, disaster, huge vessels in sea carrying cargo (metal cargo arriving at a small time frame may lead to reduce metal price in state/country).. or tesla car cargo reaching/delivering to/from some port causing possible price gain in tesla etc
all the news and their predicted impact giving buy/sell signal
technical and fundamental indicator and chart (price on chart, the most important signal)
and even news ranked in orders for helping as CDSS
correlations - (suppliers on left, the company in center and its branches below and customers on right and each having variable stake causing varying degree of impact and correlating together)
near top left (64%) -> collective intelligence, taking average of all inputs of world's best analysts.. and interesting to note none getting hundred % and rather sometime all 3 options may get equal weightage giving no decision and showing so much variability in decisions / recommendations of experts (and experts collective intelligence)
global status indicator.. combinantion of every individual trade everywhere in world in any microsecond
RB - Wow! Envision an individual health record getting updated every second globally!
Avi - could be so easy if the variety of data points were so few.. but technology may help overcome that and is already helping a lot.. we saw a glimpse of such global updating, dashboard views, and their use in prediction, planning, resource execution and various other decision making and it failed repeatedly, but not without a HUGE impact (and in some countries highly successful impact)
a cheap tool for retailers democratizing access to such cdss kind of data.. the data and evidence and analyst quality is not my point here but the access and democratization is.
various such cheap tools to do nearly everything in the costly software to some extent if not full with some troubles may be.. commenting on accuracy won't be a good thing at my stage without having a RCT with a living meta analysis
price - The cost of a Bloomberg Terminal is $24,000 per year, and terminals are leased on a two-year basis. The price drops to $20,000 per terminal per year for 2 or more terminals. while the low cost ones are like 10-20$ per year.
there are have social network kind of discussion facilities used globally i think, with other hedge fund managers, while for retailers there are many UDFCs (user drive finance care) networks on whatsapp telegram twitter and everywhere, world is connected. (UDHC = user driven healthcare - https://classworkdecjan.blogspot.com/2020/01/udhc-resources.html )
market and industry inter-relationship
RB - May need a break down of the image to simplify it for a larger audience?